The Tubercular Constitution as a Common Cause of Chronic Diseases and its Treatment with Naturopathic “Regulation Therapy”
von
Peter Schneider
(Dr.rer.nat. Dr.med.vet.)
Copyright © 2000 by Peter Schneider
It's much easier to ride the horse in the direction he's going --- Werner Erhard
Content
Historical background of the tubercular constitution
Homotoxicology according to Reckeweg
Characterisation of the tubercular milieu
Naturopathic regulatory treatment of the tubercular constitution
Historical background of the tubercular constitution
Almost 200 years ago, Samuel Hahnemann (Hahnemann, 1810, 1828) tried to classify chronic disease into certain “miasms” (disease energies). He attributed the basic toxic load to Psora (in Greek “the itch”), to Syphilis and to Sycosis (“fig-wart disease”). This work dates from the latter part of his life.
Even in ancient cultures it was recognised that all the chronic diseases that afflict mankind form a unified whole. Escaping from his opponents to Paris at the age of 80, Hahnemann tried to secure this knowledge in the 6th edition of his “Organon of the Rational Art of Healing” by adding a number of notes to the 5th edition. Due to the fierce opposition of some medical doctors to the notion of Psora, the 6th edition was only published in 1921. In that way the fanatically contested idea of Psora, which Hahnemann called the “thousand headed monster of disease” and which was dismissed as a senile fantasy of his, was handed down in its original form.
Among Hahnemann’s numerous followers John H. Allen deserves mention, for his intensive work on the theory of the miasms. (Allen, 1996). Hahnemann and his pupils had already observed that suppressive treatment of disease would intensify and increase the miasmatic disease energies. It was further realised that, when inherited, Psora and Syphilis may completely merge together. The tubercular constitution is a “mixed” miasm and a result of this merging together. Allen calls it “absolutely the strongest of all disease states or conditions”. It can be inherited or acquired and is also called “pseudo-psora”.
As the tubercular constitution does not signify a case of clinical tuberculosis, other terms such as “para-tuberculosis”, “tuberculinic” or “tubercular miasm” were introduced later. However, the term “para-tuberculosis” is nowadays used internationally, in a different sense, to denote an illness caused by Mycobacterium paratuberculosis (Johne’s disease in cattle).
Between 55 and 100 years ago clinical tuberculosis was widespread, and intensive research on it was carried out. In Berlin, Germany, Robert Koch pioneered the diagnosis and treatment (Tuberculinum Koch) of tuberculosis. His assistant Carl Spengler carried on his work and based his new methods of diagnosis and treatment of chronic illness on Koch’s findings (Spengler, 1911). Above all, Spengler’s work was concerned with the different morphology of strains of mycobacteria (“dualism”) and with the close relationship between tubercle bacteria and the pathogenic agent of syphilis, whose bacterial form is found in mixed cultures from tuberculosis patients. Spengler showed that the presence of the syphilis pathogen can be demonstrated within the cells of an organism in an ultra-small and primitive variety - even when an infection by this pathogen had never occurred during the individual’s life-time.
It was assumed that the general spread of “inherited syphilis” stems from the beginning of the 16th century, when a whole population was infected with a syphilis pandemic “imported” from America. Anyone who did not die of this infectious disease at that time, retained a residual toxicity in the body that was passed on through generations and, according to Spengler, would later show up as an “inherited virus”.
Spengler developed the so called “Spengler colloids” which were named after him and are antigens from different bacteria and anti-toxins produced from the blood of highly immunised rabbits. With the help of these substances it is possible to diagnose various chronic diseases such as the “inherited toxins” of tuberculosis and syphilis (see POLYSANS, produced by the SANUM-KEHLBECK Co).
In a study on trans-placental carcinogenesis in mice, an extra-chromosomally transmitted susceptibility to tumour growth could be observed (Schneider, 1981). In the F2-generation only those animals showed an increased occurrence of tumours, whose parent of the same sex had been transplacentally exposed to the chemical carcinogen (DMBA) and had been crossed with a non-treated animal. This dependency on the sex and trans-placental exposure regarding tumour formation permits the assumption that extra-chromosomal influences are at work.
By the end of the last century the French chemist and pharmacist Antoine Béchamp had claimed (Béchamp, 1912), that certain micro-organisms could occur in various forms and stages of development. Under exactly defined conditions they would occur, ranging from the lowest forms to the highly developed stages of bacteria and fungi. He found that all animal and plant cells contain minute granules (“microzymas”), which do not perish after the death of an organism, are responsible for fermentation, and from which other micro-organisms could also develop. These microzymas would be present in every living species, in humans, animals and plants; they were eternal and indestructible and represented a bridge between non-living and living matter. Under certain or pathogenic influences these microzymas could develop into bacteria with putrefacient and fermenting properties. This meant that disease had its origin mainly within the body.
In the year 1997 Stanley Prusiner won the Nobel Price "for his discovery of prions - a new biological principle of infection". These prions are probably nothing else than the micozymas which were discovered by Béchamp about 100 years earlier.
Claude Bernard, a French physiologist and a contemporary of Béchamp, confirmed his results and found out in addition that not only the micro-organisms themselves are harmful, but primarily the “soil” in which they multiply.
Another contemporary of theirs at the end of the nineteenth century was Louis Pasteur. He claimed that the explanations of Béchamp and Bernard were arrant nonsense. He contested these views in accord with the botanist Cohn (Breslau) and Robert Koch’s theory of “monomorphism” (meaning that each type of bacteria is only allowed one mode of growth and manifestation). His opinion prevailed among the experts of his time and still does so even in modern times. Nevertheless Pasteur said on his death bed: “Bernard is right; the soil is everything, the microbe nothing”. Pasteur’s private notes about his scientific research were kept secret from the general scientific community at his request. Not until 1975 were 10,000 pages of his laboratory protocols handed over to the historian G. L. Geison at Princeton University, who spent almost 20 years evaluating them. In 1993 Geison handed over his results to the American Association for the Advancement of Science in Boston. In 1997 a book containing Geison’s findings was published. (Geison, 1997). This book shows Pasteur’s merits, but does not cover up the fact that that he manipulated some of his experimental results and contravened medical, scientific and ethical rules.
Fontes (Fontes, 1910) who had based his research on Spengler’s results, delivered important proof of the “pleomorphism” of bacteria. He was the first to provide proof of the infectiousness of bacteria-free filtrates of TBC-bacterial cultures. As a result of his research Fontes assumed that not only the predisposition to tuberculosis could be inherited, but also the virus in its “filterable”, granular form. He further thought that the latter could remain latent (“latent tuberculosis”) or could develop slowly into the classic bacterial type.
G. Enderlein (zoologist and microbiologist, curator of the zoological museum of Berlin University, and microbiologist for the German army in Stettin during World War I) reported in 1916 for the “Friends of Natural Research”, Berlin, about his time as a bacteriologist in the army and his research results regarding the development of bacteria. Owing to the prevailing conditions resulting from the war, his monograph on this subject was only published in 1925 (Enderlein, 1925). As he was describing morphological facts that had previously been unknown to microbiology, he developed a whole new terminology; however, this resulted in the procedures he described being difficult to understand.
According to Enderlein, microbes pass through a cycle which is specific to their species. The term “cyclogeny” describes the changes and the journey of pathogenic and non-pathogenic micro-organisms through all phases (“valencies”). The cycle starts below the limits of microscopic visibility, the viral sphere, then on via forms of higher valency like cocci and bacilli, to culminate in the fungal phases. The bacterial nucleus (“mych”) has a special significance. Although this was already known before Enderlein, its function had not been interpreted accurately. According to the “basic Anatartic Law” fomulated by Enderlein, the increase in valency of the microbe depends on the “milieu” that is present in blood and tissues, which is mainly characterised by its pH value. Bacteria can either multiply asexually by division or branching (“auxanogeny”) or sexually after prior fusion of cell nuclei (“probćnogeny”). Sexual multiplication is essential for movement to a higher or lower phase. 40 years after Enderlein’s discovery, the Nobel prize was awarded to Lederberg in 1958 for discovery of “polymorphy” and sexual multiplication of bacteria by the fusion of cell nuclei (Lederberg, 1958).
Apart from naming the various phases in the development of micro-organisms, Enderlein also succeeded in proving the existence of the most important symbiont (“endobiont”) in warm-blooded creatures. He discovered Mucor racemosus Fresen(ius) 1870, in all its developmental stages from viral to fungal. In the low valency stages, the endobiont lives as a physiological regulator; in the higher valency stages it will develop pathogenic characteristics, depending on the environment (or milieu) that surrounds it. Changes in the environment which are followed by an endobiosis occur in all chronic illnesses. The endobiosis caused by Mucor racemosus in a higher-valency form is characterised by congestive symptoms (e.g. diseases of the blood and venous system, wounds, hearing loss and neurodermatitis).
Enderlein also found that the pathogenic higher-valency phases of the endobiont could be reconverted into a non-pathogenic phase by introducing low-valency forms while simultaneously treating the milieu (“isopathic therapy”). These processes can be observed with the help of dark-field microscopy of vital blood. (Schwerdtle and Arnoul, 1993; Bleker, 1997).
According to Enderlein, viruses are cell-free primitive forms (“filum”) of the endobiont, from which bacteria may be grown. (For example: the tobacco mosaic virus, from which it was possible to breed bacteria after several months); bacteriophages however are “spermits” of the microbes (Enderlein, 1954).
The causative agent of the second electively pathogenic endobiosis which, in contrast to the Mucor symbiosis, is non-physiological, was identified by Enderlein as the mould Aspergillus niger van Tieghem. In its polymorphy and phase-dependent pathology this is believed to be a causative agent of cancer (Dechow, 1933) and tuberculosis. Vaudremer (1921) and Tissot (1925) had already found a genetic connection between the tubercle bacillus and fungi of the species Aspergillus (according to Enderlein, 1949).
The cyclode of Aspergillus niger, according to Enderlein, is a scission from the cyclode of Mucor racemosus (Figure 1).
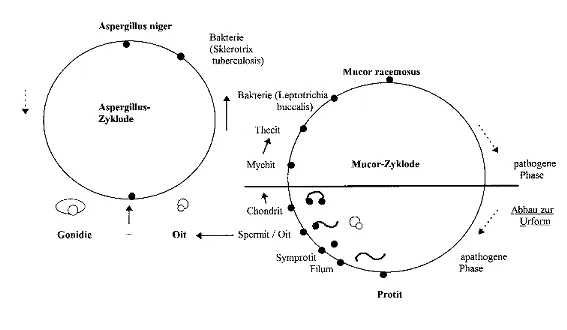
Figure 1: Hypothetical separation of the Aspergillus niger cyclode from that of Mucor racemosus
(Arnoul, 1998; Rau, 1998)[The cyclogenies of Mucor racemosus and Aspergillus niger
Bakterie = bacterium
Mucor-Zyklode = Mucor cyclode
Aspergillus-Zyklode = Aspergillus cyclode
Pathogene Phase = pathogenic phase
Apathogene Phase = non-pathogenic phase
Abbau zur Urform = deconstruction back to the original form]
According to Enderlein, the low valency phases of Mucor racemosus and Aspergillus niger are transmitted via the placenta.
The higher and high valency phases of Aspergillus are closely connected with calcium metabolism and cell respiration (citric acid cycle) and they cause chronic tubercular diseases in warm blooded creatures “to the right of the biological incision” (Reckeweg, table 1). Examples are chronically relapsing susceptibility to infections, tuberculosis, paratuberculosis, asthma, arthrosis, ankylosing spondylitis, cysts, ovarian and prostate diseases, as well as cancer. Among the tubercular symptoms degenerative diseases such as auto-immune disorders may also be found.
The particular significance of high-valency fungal forms in the development of neoplastic disorders was confirmed by Privy Councillor Prof. Dr. F. Gerlach, Director of the Bundesanstalt für Tierseuchenbekämpfung (National Institute for the control of epidemics among animals) in Mödling near Vienna, following detailed research. Gerlach was able to culture fungi from cancerous material of human or animal origin (including chemically induced tumours from animal testing) at every attempt (Gerlach, 1948). Later he also found that mycoplasma play an important role in carcinogenesis. From this it may be assumed that mycoplasma which, according to Mattman are barely distinguishable from CWD-types (see below), are higher valency forms of the Aspergillus-cyclode.
Tubercular diseases were given various names by Enderlein’s contemporaries, without acknowledging any connection to the bacterial cycle. Scrophula, lymphatism, camouflaged tuberculosis (Patromikolas), masked tuberculosis (Willy Bircher), certain forms of rheumatic disease (Poncet), latentia, tubercular toxicosis, paratuberculosis. "Much’s Granules" and "Spengler’s splinters" also belong in this category.
The “Basit”, “Linit”, and “Ascit” stages of Aspergillus are the short and long bacilli of Sclerothrix tuberculosis Koch 1882, acidoresistant and non- acidoresistant, the cultivation of which was described by Enderlein in all its phases (Enderlein, 1959).
After Enderlein, Harmsen also described forms of Mycobacterium tuberculosis which deviated from the slender bacillary form: branched varieties, granula, acidoresistant and non-acidoresistant forms, mycelium formation, nuclear equivalents and vacuole formation (Harmsen, 1952).
Just as the low-valency phases of Mucor racemosus are especially suited to the treatment of endobiosis, so tubercular diseases can be treated very effectively isopathically with low valency phases of Aspergillus niger. According to Enderlein the Aspergillus-cyclode is an off-shoot from the Mucor-cyclode and therefore the medicine is also prescribed in a combination from both cyclodes.
An extensive survey of the numerous studies on polymorphic “symbionts”, particularly in German speaking countries, was carried out by Windstosser (Windstosser, 1995) .
In English-speaking countries too, intensive research on the pathogenicity of polymorphic forms of microbes has been carried out during the last 40 years. Probably because of the language barrier, the results of earlier research remained unnoticed. Only in recent times has an effort been made by Canadian research groups to pool this knowledge (First International Symposium on Pleomorphic Microbes in Health and Disease, 18th-19th June 1999, Montreal, Canada).
The existing investigations on the properties and pathogenicity of the so called “Cell Wall Deficient Forms” (CWD) were recently summarized by Lida H. Mattman, Emeritus Professor of Microbiology at Wayne State University, Detroit, Michigan (Mattman, 1993).
“CWD” is used as the umbrella term for synonyms like “L-forms”, “L-phases” or “spheroplasts” that can be found in the literature. CWD also covers the previously used term “protoplast”. Figure 2 shows cell wall deficient bacterial forms of the blood under a dark-field microscope. The elements with the thick, white peripheral zones are erythrocytes.
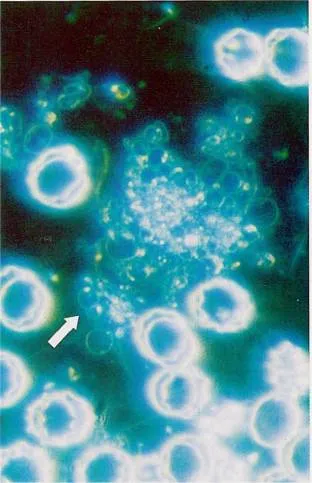
Figure
2: CWD ("Mychite") in vital blood under the dark-field microscope
(from Bleker, 1997)
CWD have special characteristics that are not present in classical micro-organisms:
Destruction of many forms during fixation with heat;
they usually require soft agar, grow under the surface and need a mature, autoclaved culture medium;
they typically grow within erythrocytes;
they are often serophilic;
most types grow best in a hypertonic and alkaline environment (ph 7.8 – 8.0);
CWD are able to revert to classical bacterial forms.
It is only possible to culture CWD under special conditions. The culture medium has to be stabilised with an extract of heart muscle, 15% inactivated horse serum and 3.5% sodium chloride.
The following are some examples of the intra-erythrocytal growth of CWD:
normal and physiological |
Staphylococci, Bacillus licheniformis (in approx. 30% of all healthy humans) |
Sarkoidosis |
Mykobacteria |
Kaposi's sarkoma |
Fungi |
Nephropathy |
Lysis of erythrocytes from 489 patients: the same species as in urinary infections |
Idiopathic hćmaturia |
Bacteria similar to streptococci; in contrast to this, children with nephrotic syndrome exhibited an elevated staphylococcal growth-rate |
Systemic lupus erythematosus |
Bacteria connected with nephrotic diseases |
Crohn’s disease |
Pseudomonas, mycobacteria |
Auto-immune diseases |
CWD act as haptens and stimulate the formation of haemolytic antibodies (Example: paroxysmal hćmoglobinuria due to cold in syphilitics) |
The formation of pathogenic CWD from bacteria can be induced by suppressive treatment. in-vitro their formation is possible through antibiotics, e.g.:
Penicillins |
Inhibition of murein synthesis: Brucella, Clostridia, E. coli, Haemophilus influenzae, Listeria monocytogenes, Proteus mirabilis, Salmonella gallinarum, S. typhi, Vibrio cholerae, Vitreoscilla. |
Streptomycin |
Mycobacteria (e.g. Mycobacterium tuberculosis and Mycobacterium paratuberculosis) |
Sulfonamides |
Staph. aureus |
Kanamycin, |
Inhibition of protein synthesis, resulting in surface changes in bacteria: E. coli, Klebsiella pneumoniae, Bacillus megaterium, B. polymyxa, Serratia marcescens, Sarcina lutea, Staphylococcus aureus, Salmonellen, Shigellen, Proteus |
Aztoreonam |
(Monobactam) surface changes in E. coli |
Erythromycin |
Staphylococcus aureus (and at least 40 other macrolid-antibiotics such as Leukomycin, Oleandomycin, Spiramycin, Tylosin) |
Tetracyclines |
Staph. aureus, E. coli, K. pneumoniae, B. megaterium, B. polymyxa, Serratia marcescens, Serratia lutea, Salmonellć, Shigellć, Proteus |
As an example of an in vivo induction of CWD by antibiotics Mattman names antibiotic treatment of mastitis in cows caused by Staphylococcus aureus:
- apart from the classical bacterial forms, the CWD of Streptococcus agalactiae, Staphylococcus aureus and Corynebacterium pyogenes were also demonstrated as causative of bovine mastitis (Bergmann and Böckel, 1989).
- following treatment of mastitis caused by Staphylococcus aureus with Cloxacillin the excretion of classical forms of cocci ceased within a few days, whereas CWD forms of Staph. aureus continued to contaminate the milk for more then 30 days (Sears, P.M. et al., 1987).
Nowadays the induction of pathogenic CWD in vivo by using antibiotics is of great importance as antibiotic-resistant micro-organisms are widespread and can no longer necessarily be destroyed (Beyer, 1999). On the other hand CWD commonly escape from the immune system due to their lack of a cell wall and continue to act as haptens. To support the organism in the elimination of cell wall deficient microbial forms, the SANUM-therapy which includes SANUKEHL preparations should be the treatment of choice. (Schneider, 1999a; Werthmann, 1999).
On the basis of clinical research to date it can reliably be asserted that:
Micro-organisms can be of a polymorphic phenotype, from the smallest viral structures to bacteria and fungi.
CWD of micro-organisms (staphylococci and bacilli) appear physiologically in the erythrocytes of healthy humans.
Cell wall deficient forms can occur in vitro and in vivo under certain environmental or “milieu” conditions and can be pathogenic in vivo.
CWD pathogenic forms can live as parasites within erythrocytes and can be observed in vital blood under a dark-field microscope.
Suppressive treatment of disease, especially with antibiotics, can induce the development of CWD.
Cell wall deficient forms of mycobacteria are the real carriers of a tubercular constitution.
CWD are able to revert to classical forms of bacteria. According to Enderlein they can move through their cyclodes in both directions.
Pathogenic forms of micro-organisms can be rendered harmless when transformed into their non-pathogenic regulatory forms.
Homotoxicology according to Reckeweg
According to Reckeweg (Reckeweg 1975, 1980) the body’s “major defence system” consists of 5 different mechanisms (reticulo-endothelium, anterior pituitary-NNR-mechanism, nerve reflexes, liver detoxification, detoxifying function of connective tissues) by which the body defends itself against toxins (“homotoxins”), which can otherwise bring about illness. Either the body wins in this fight and gets damaged in varying degrees by the homotoxins or it succumbs to the toxic effects.
These views of Reckeweg’s are an extension of Selye’s research on the Adaptation Syndrome (Selye, 1953).
The damage caused by the homotoxins manifests in the form of an impairment or blockage of the intracellular enzyme systems. In Reckeweg’s system, the different grades of toxic effects are expressed as six different phases. During the first three phases (excretion, reaction, deposition) the excretion of toxins is successful, whereas during the three cellular phases that lie beyond the “biological incision” (impregnation, degeneration, neoplasm) the cells are increasingly damaged and become more or less non-functional. The three cellular phases often result from the suppression of acute illnesses. Numerous chemically defined substances such as antibiotics, anti-rheumatic drugs, analgesics, bacteriostatics among others, according to Reckeweg often have an irreversible blocking effect on the intracellular fermentation systems and bring the cellular phases four to six into play (“progressive vicariation”). These phases correspond to the terms “psora” and “sycosis” which were originated by Hahnemann, or with the “tubercular constitution”. According to Reckeweg’s six-phase scheme (table 1), clinical tuberculosis only appears in the degeneration phase.
The following authentic case example will serve to clarify the term “progressive vicariation”. The patient is a young male whose medical history began in infancy as a “dysbiosis” with an acute, inflammatory, excretory reaction and developed over 16 years into a degenerative demyelinisation of the central nervous system:
Age |
Disease |
Treatment |
2 months |
Pre-toxicosis with Coli-Dyspepsia, diffuse peri-bronchitis, high fever |
antibiotics i.v.and i.m., milk-based “health-food”, fluoride |
4 months |
Super-infected varicella, anal fissures, streptococcal sepsis, high fever |
antibiotics, antipyretics, |
5 months |
Coli-dyspepsia, chickenpox, diarrhśa, vomiting |
antibiotics, immuno-globulins, |
1 year |
superinfected
intertriginous eczema, eczema
of scalp, infection of lungs (mild), |
antibiotics, antifungals, |
14 months |
histiocytosis X, constipation |
chemotherapy, prednisolone |
2 years |
histiocytose X, recurrent focal of infection on right side |
chemotherapy, corticoids |
6 years |
accident |
tetanus vaccination |
7 years |
loss of teeth after chemotherapy |
|
14 years |
Cerebellar ataxia, hydrocephalus int., anal fistula, kyphoskoliosis, dwarfism, anus prćter, mental and motor retardation |
valve implant owing to hydrocephalus |
16 years |
increasing muscular dystrophy, nystagmus, astigmatism, demyelination in pons and und mesenzephalon, strabism, unable to walk after steriotactic biopsies, patient confined to a wheelchair |
further attempts at corticoid treatment; aborted after onset of Cushing’s syndrome and aggravation of acne |
According to Reckeweg the aim of a biological therapy is to enhance detoxification and excretion via the major defence mechanism. The reactivation of the damaged or blocked enzyme systems by administering adequate co-factors such as vitamins, trace elements, intermediate citric acid cycle catalysts and quinones is of the utmost importance. A biological therapy also aims to transform the “dangerous” phases on the right side of the biological incision into less harmful phases (“regressive vicariation”). An example is the induction of inflammatory reactions in neoplasma phases.
Reckeweg concludes that all natural healing operates according to the principle of regressive vicariation. The individual phases of the pathogenesis are briefly re-experienced in the reverse order of their appearance, beginning with the most recent events. This means that during recovery apparently new illnesses seem to appear (e.g. appearance of acute herpes during the treatment of a degenerative disease). Under no circumstances must these symptoms be suppressed. In such cases relief can be obtained by intensifying the use of excretory measures, by giving a classical homśopathic remedy that is indicated for a certain stage of illness, or by acupuncture.
Table 1: Homotoxicosis: 6-phase Table, after Reckeweg, 1975
Tissue
Humoral Phases
Diseases of DISPOSITION
B
i
o
l
o
g
i
c
a
l
i
n
c
i
s
i
o
nCellular (tuberculinic) phases
Diseases of CONSTITUTION
Excretion
Reaction
Deposition
Impregnation
Degeneration
Neoplasma
Ectoderm
Saliva
Dermatitis
Warts,
PolypiMigraine,
LeucoplakiaChronic
dermatitisBasalioma
Nasal
catarrhRhinitis
Atheroma
Multiple
sclerosis,
EpilepsyLupus,
PsoriasisAdenoma
Sweat
Furuncle
Cataracta
senilisAsthma,
Hay feverCushing’s
syndromeMelanoma
Tears
Stomatitis
Incipient
asthmaRhinitis
atrophicansM.S.,
Parkinson’sSarcoma
Herpes
zoster,
NeuralgiaUlcus
ventric./duod.Meničre’s,
AlzheimerEntoderm
Intestinal
juicesColitis
syndromeConstipation
Asthma
Tuberculosis
Carcinoma
of pancreas,
gall bladder,
intestinesBile
Enteritis
Megacolon
Ulcus
ventric./duod.Diabetes
mellitusMyeloma
Pancreatic
juiceParotitis
Struma
Recurrent
infectionsCirrhosis
of liverSarcoma
Hepatitis
Silicosis
Chronic
tonsillitisCholangitis
Cholelithiasis
Mesenchym
Antibody
productionOedema
Adiposity
Lymphatism
Tuberculosis
Sarcoma and
carcinoma
of kidneysVicarious
bleedingAbscess,
UlcerGout
Elephantiasis
Scleroderma
Menstruation
Angina
Lymph node
swellingsIncipient
agranulo-cytosisFibroma
Sarcoma and
carcinoma of
serous
membranesTyphus
Otosclerosis
Uterine
carcinomaAppendicitis
Lipoma
Paradontosis
(final stage)Myosarcoma
Polyarthritis
Exostosis
Leukćmia,
LymphomaMesoderm
Lactic acid
productionCystitis
Myogelosis
Hydro- nephrosis
Exhaustion
(Selye)Carcinoma of skin and genitals
Discharge
of serous membranesPyelitis
Myalgia
Prostages
of tumoursTuberculosis
Nephritis
Rheuma
Atrophic
kidneyProstatitis
Cysts
Muscular
dystrophySalpingitis
Muscular rheumatism
Excretion principle; prognosis favourable
Condensation principle; prognosis doubtful
Characterisation of the tubercular milieu
By “the milieu of the tissues” we mean the “cell milieu system”, whose properties have been described by Pischinger (Pischinger, 1990).
Changes in the milieu can be characterised on various levels, for instance by dark-field microscopy or on an electromagnetic level with the aid of Vincent’s system of Bio-electronics (BEV).
In the dark-field microscopy hćmogram of native blood changes may be observed in the morphological structure of erythrocytes related to their position on the right side of the “biological incision”. The observations extend from changes in the shape of erythrocytes to forms similar to a “thorn apple” (see Figure 3; Schwerdtle and Arnoul, 1993; Bleker, 1997). These structures have been described, documented and named by Enderlein and they can easily be reproduced. For dark-field microscopy examination a special microscope is required.
Figure 3: moderate (left) and strong (right) infestation of native blood with endobionts (from Bleker, 1997)
Another possibility for the characterisation of the milieu is afforded by Vincent’s system of Bio-electronics (BEV).
As was already known 100 years ago, the most important parameter for a milieu is the pH (Worlitschek, 1996). The pH represents the ion-potential for acidity and alkalinity and is the “magnetic factor” according to Vincent. The pH value is 7.40 - 7.45 in arterial blood, 7.35 - 7.40 in capillary blood, and in venous blood 7.30 - 7.35. An average blood pH of 7.2 is regarded as normal, but nowadays this is rarely attained. Based on regulatory reciprocal actions, the blood pH works in the reverse direction to that of the tissues, so that a blood pH of 7.5 is equivalent to a tissue pH of approx. 5.5. According to Enderlein the endobiont develops in the blood at a pH of 7.20 - 7.50.
Another important milieu parameter is the redox-potential. The significance of this parameter was discovered by the American doctor W.F. Koch (Koch, 1981). Koch was a physiologist and pathologist and from 1919 to 1949 he was director of the Koch Cancer Clinic in the USA. He introduced homśopathically prepared (6X or 9X) substances that contain carbonyl-groups such as glyoxals and quinones into cancer therapy and had to defend himself before American courts due to his innovative methods of treatment. As his results were brilliant, he was scarcely troubled by such accusations.
Koch assumed that pathogens such as viruses and antibiotics would be “anchored” in the metabolism as they reacted with amino-groups such as those of creatinine and formed polymers, which would primarily impair the function of the respiratory chain. He guessed that the hypoxia that was created in that way was the reason for the development of cancer and other illnesses. Therefore Koch developed homśopathic preparations with a high redox potential in order to overcome this hypoxia and to disperse the anchored pathogens.
Until now it has not been possible to verify the mechanism by which his preparations work, but Mäkinen and Mäkinen (Mäkinen and Mäkinen, 1982) were able to demonstrate within a biological system that the substance methylglyoxal has “photo-enhancing” properties at a wave-length of 300nm. Apart from Glyoxal, Methylglyoxal was the most important of the substances employed by Koch.
It has long been known that essential metabolic processes are dependent on emission of quanta of light. It used to be assumed that this was merely a side-effect of chemical processes, but the German physicist Popp, employing considerable technical resources, proved that photons are of the greatest importance for inter-cellular communication (Popp et al., 1992). The light emitted by living cells in the form of biophotons is very weak (low-level luminescence). However, within a healthy organism, it shows a very high degree of coherence, similar to a laser, and therefore has a high quality of resonance.
As early as the 1920’s, communication by means of light between the roots of two onions had been observed by Gurwitsch. In 1928 Reiter and Gabór of the Siemens research laboratory in Berlin showed that the radiation wavelength of this communication lies in the ultra-violet area of the spectrum at exactly 338nm. It was of particular significance that this radiation could be antagonised by weak light with a wavelength of exactly 300nm. This was exactly the same wavelength at which Mäkinen and Mäkinen had also found biological properties. Popp proved that, in neoplastic disease, the intensity of the photon emission is reduced. The same applies to its organisation (coherence). Cells from induced tumours of laboratory animals had largely lost their light contact, as compared with normal cells. On the basis of experience with medicines which are obviously able to influence photon emission, their properties also seem to be altered in other chronic diseases.
In the light of the photon research we may assume that the administration of Koch’s homśopathic remedies causes the cells to increase their emission of light and therefore contributes considerably to the restoration of the organism’s regulatory abilities. For the treatment of chronic illnesses a combination of Ubiquinone comp. (Heel) with CITROKEHL in a mixed injection has proved especially valuable. This combination not only stimulates photon emission, but also cellular respiration.
Apart from a modification of the redox potential to an “electrical factor rH2” (rH2=2 x pH + 30 x E [electron potential in mV]) the French hydrologist Vincent introduced the conductivity and it’s reciprocal value, the specific electrical resistance r [Ω] as a third essential milieu parameter (Elmau, 1985). Like pH and rH2 these originally served to determine the quality of water, but it soon turned out that these three measuring units are equally suited to the evaluation of biological substrates. Vincent expanded the evaluation of the milieu to include the simultaneous measurement of the parameters in blood, saliva and urine.
With the help of these three parameters it is possible to show four quadrants of the biological milieus for the blood (Figure 4):
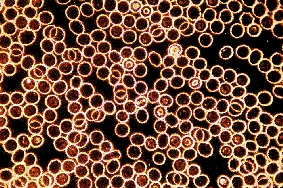

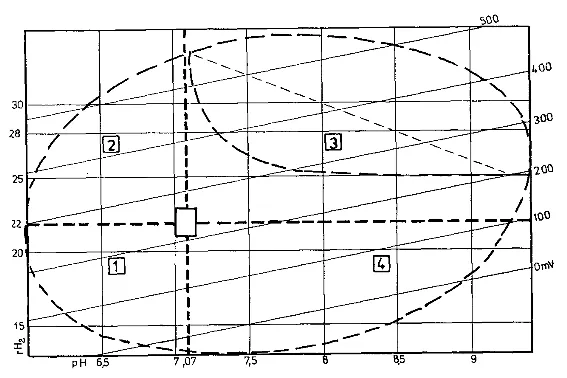
Figure 4: Vincent’s bioelectronics - the four zones of the biological terrain in the blood
(from Elmau, 1985)The small box between the quadrants indicates the area of health.
Quadrant 1: acidic – reduced
favours the healthy living of higher organisms; it is the terrain for e.g. green algć, simple microbes and symbionts.
Quadrant 2: acidic – oxidised
Has a disposition towards bacterial infections and to fungal infestation; is the terrain for e.g. lichens and fungi, therefore also for mycoses, tubercle- and leprosy bacteria as well as antibiotic forms of fungi.
Quadrant 3: alkaline – oxidised – hypertonic, which is the area of the tubercular constitution
It is precisely the area of chronic disease in which pathogenic cell wall deficient bacterial forms (CWD) prefer to grow, according to Mattman. It is characterised by increased release of free radicals and, according to Vincent, disposes the patient to chronic viral diseases and degenerative processes (c.f. Inoue u. Suga, 2008). The dotted, downward-curving line which is curved downwards within this quadrant marks the area of malignant diseases; the diagonal line within this quadrant is the “line of thrombosis”.
Quadrant 4: alkaline – reduced
Finally, this is the terrain for pathogenic germs such as pneumococci, typhus, cholera, the plague, as well as for kelp.
Within quadrant number 1 a normal healthy life is possible. Approximately a hundred years ago the frequent occurrence of clinical tuberculosis was very characteristic; the condition of the blood at that time often corresponded to quadrant number 2. While living conditions changed during the last 50 years, a further move towards quadrant number 3 has taken place. Therefore nowadays the classical bacterial infectious diseases are rarely seen and, in their place, chronic viral diseases are on the increase, and so are degenerative and malignant processes. Mycoses, which are frequently seen these days, indicate a transition from quadrant number 2 to number 3.
Looking at the changes of the blood milieu towards quadrant number 3, which is the quadrant of chronic illness from the bio-energetic point of view (table 2), it becomes clear that in contrast to the physiological conditions a marked increase of energy takes place in the blood. However, as cell metabolism is blocked, this energy cannot be put to use by the tissues. For that reason energy in the saliva is decreased and only a fraction of the energy is excreted with the urine, compared to the normal amount.
Owing to these changes in the milieu of blood and tissues serious changes take place in the basic system according to Pischinger. Based on the energetic changes in the blood in chronic disease, it can be assumed, that sufficient energy is present to ensure the survival of cell wall deficient bacteria and cytoplasm. Like viruses they do not need their own energy metabolism due to their parasitic life-style within erythrocytes and leucocytes, but simply require the equivalent of their cell nucleus.
Table 2: BEV-values and their energetic capacity in blood, saliva and urine under physiological and pathological conditions (calculation based on BEV-values)
Ideal values
pH
rH2
E
r
Effort [µW/cm3]
Blood
7.10
22
234
210
261
Saliva
6.50
22
270
140
521
Urine
6.80
24
312
30
3245
Strong pathological values
pH
rH2
E
r
Effort [µW/cm3]
Blood
7.50
25
300
121
744
Saliva
7.25
26
345
310
384
Urine
4.80
19
282
127
626
Should the pathological changes in the blood and body tissues of the population continue as previously and unchecked, it is very likely that the blood milieu will move into quadrant number 4. In this quadrant life as we know it today will probably no longer be possible. Incidentally, the condition of our pets and domestic animals is not so different from that of humans. Comparable milieu changes in the interior and exterior of plants also play a part in the development of plant diseases (Hoffmann et al., 1994). This shows quite clearly that humans, animals and plants are all part of one common ecological system.
The most important factor for milieu changes in humans is nutrition (Mielke, 1998); of especial significance is a high intake of animal protein. Furthermore vegetable foods only deliver a fraction of the nutrients that they used to contain a few decades ago as the soil in which they are grown is depleted.
As long as 30 years ago Kollath (Kollath, 1967) pointed out the result of an ongoing deficient diet (“mesotrophy”): “The situation is very simple: Following a diet rich in animal protein as recommended by Kühnau for younger as well as older people, those who follow this diet will move towards chronic illness and infirmity ‘irrestibly and irrevocably’, to use Kühnau’s own words. If we can manage to convince people of the importance of a diet based on wholefoods, as I have suggested, then it will be possible gradually to regain the original state of health of individuals and that of following generations”. Animal testing carried out on rats with a “scientific diet” had shown that the results of chronic malnutrition can get dramatically worse over only a few generations. This will show itself in the shape of malformations, stillbirths and finally extinction after the 4th generation.
As we know today, chronic malnutrition leads first to chronic intestinal inflammation with dysbiosis and, later, to a degeneration of the intestinal mucosa with atrophy of the villi (Werthmann, 1988a) and finally to the so-called “Leaky Gut Syndrome”. This means that the intestinal mucosa becomes increasingly permeable to macro-molecules of the lumen, antigens and toxins, connected with an inflammatory-degenerative and/or atrophic destruction of the mucosa. As a result of the damage to the intestinal walls, the function of the gut as an excretory organ is seriously compromised. According to estimates in the USA, approximately 40% of the population there currently suffer from leaky gut-syndrome.
Taking the chronically inflamed and degenerated gut as a major cause of the tubercular milieu, we find that it has seven pathogenetic aspects:
1. Malabsorption of nutrients followed by flatulence and tiredness.
2. Absorption of large food particles leading to food allergies and new symptoms in the target organs
like arthritis and fibromyalgia.3. Damage to the carrier proteins resulting in a relative nutritional deficiency which can bring out a
variety of symptoms, such as magnesium-deficiency-related muscle spasms or copper-deficiency-
related elevated cholesterol values.4. Impaired detoxification via the gut resulting in an increased sensitivity to chemicals (MCS).
5. Impaired defence by immunoglobulin A, leading to a lowered immunity to protozoa, bacteria,
viruses and Candida.6. Bacteria and yeasts can penetrate the gut wall resulting in infection of body cavities and organs.
7. Formation of antibodies, which can penetrate the gut wall and resemble antigens of our own tissues,
resulting in auto-immune diseases such as rheumatoid arthritis, lupus, multiple sclerosis, thyreoiditis
and other “incurable” diseases.As approx. 80% of the body’s immunologically active tissue can be found in the intestinal area, the tubercular milieu has a direct impact on the immune system. According to the American Food Marketing Institute, there is therefore a close relationship for the U.S.A. between diet and frequency of illness. (Source: Food Marketing Institute, USA, quoted by Reimerdes):
High Cholesterol |
93 % |
Cardiac diseases |
88 % |
High blood pressure |
86 % |
Stroke |
69 % |
|
Diabetes |
65 % |
Intestinal cancer |
60 % |
Prostate cancer |
35 % |
Breast cancer |
30 % |
Apart from diet, other influences may be of significance in the development of a tubercular milieu, such as disturbance fields, of which up to approx. 80% are located in the head area (particularly in teeth, sinuses, tonsils) or psychological factors. Disturbance fields or a heavy metal toxic load (e.g. amalgam from dental fillings) are the most common barriers to recovery in naturopathic therapy (Kobau, 1998). Figure 5 shows the relationship of various organs to the teeth.
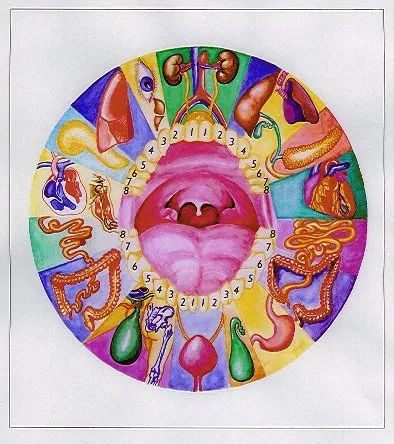
Figure 5: Relationships
between teeth and organs
(Copyright © 1998 by MUDr. Josefa Jonáše)
Most important are generally suppressive treatment interventions and vaccinations (Elmau, 1985); these can alter the milieu so permanently that the metabolism is driven further into the tubercular constitution.
One example is diabetes mellitus which is a degenerative disease of the tubercular constitution. It is clear that a marked increase in this illness has occurred especially in elderly American patients during the last 40 years (Figure 6). These curves run broadly parallel with those for other tubercular diseases and they also run parallel to the introduction of antibiotics, chemotherapy and vaccinations (Vithoulkas, 1998).
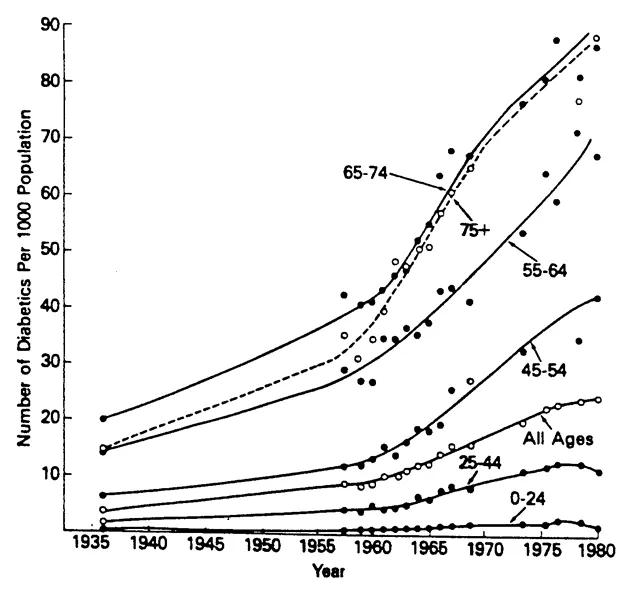
Figure 6: Trends in the prevalence of diagnosed diabetic patients of different age-groups in the USA since 1935 (Harris, MI, National Diabetes Data Group, from data of the National Health Interview Surveys, National Center for Health Statistics, 1984) from F.A. Gries (1991)
Naturopathic regulatory treatment of the tubercular constitution
Conventional medicine doubtless has its merits, and the aim of this article is not to disparage it. However, if medications are used which are known to favour the development of the tubercular constitution and therefore of chronic illness, the damage caused should be addressed by using naturopathic treatments in order to minimize the negative effects. Examples of such medications are vaccines, antibiotics and chemotherapy. Otherwise the widespread tubercular constitution and the anticipated move of the blood milieu into quadrant 4, according to Vincent, could signify a serious threat to the health of the population.
In conventional medicine, clinical tuberculosis is treated by combinations of anti-tubercular drugs. For other tubercular diseases such as cancer, even today surgical and chemotherapy measures are applied in many cases. However, gradually the realisation seems to be dawning that there are metabolic mechanisms that make a regulatory treatment of cancer possible.
Recently the results of a multi-centred study about the risk of melanoma were presented; this had been carried out with the support of “Deutsche Krebshilfe” (Project-No. 70-2112) (Kölmel et al., 1999). It was found that the “risk of suffering from a malignant melanoma decreases if an individual has experienced recurrent febrile infections”; “the risk of melanoma was significantly lower when the questioned individuals had had tuberculosis, severe staphylococcal infections (e.g. in the form of abcesses, inflammation of the mammary gland or of bone marrow), blood poisoning or pneumonia. The risk was also reduced when the questioned individuals had had a minor infection with fever above 38.5 degrees C, such as influenza, bronchitis, herpes or summer diarrhśa in the previous five years. The more infections the investigated individuals had had, the lower was their risk of suffering from melanoma. (Quote from a press release of the “Deutsche Krebshilfe”, 1999).
These are things that practitioners of natural therapies have known for a long time.
Apart from the removal of obstacles to cure and a change to a wholesome diet, a naturopathic treatment of the tubercular constitution according to the guide lines laid down by Vithoulkas (Vithoulkas, 1998) should be undertaken.
Based on the investigations by Kollath and others, a fully nutritional diet consists of the following: (modified from v. Koerber et al., 1987):
Preferably food of vegetable origin (predominantly lacto-vegetarian diet)
Preferably unprocessed food ( food should be as natural as possible)
Ample consumption of uncooked fresh foods (approx. half of the total dietary intake)
Preparation of tasty meals by using fresh, gently cooked food with only small amounts of fat
Avoidance of foods that contain additives
Avoidance of food that has been processed by certain technologies such as genetic modification, food design, irradiation
If possible only using products of approved organic farming (according to the guide lines of each country e.g AGÖL or IFOAM)
Preferably regional and seasonal products
Food preferably unpackaged or wrapped in an environmentally friendly way
Avoidance or reduction of the general emission of pollutants and therefore of intake of pollutants by using environmentally friendly products and technologies
Reduction of depletion from refining, by reducing intake of animal foods; no meat from pork, hare or rabbit (Reckeweg)
Preferably agricultural products grown and marketed under socially acceptable conditions (e.g. fair trade with developing countries).
These recommendations were further amplified by the pćdiatrician and general practitioner Konrad Werthmann (Werthmann, 1997), who generally recommended abstinence from cow’s-milk-derived protein and chicken’s eggs.
Owing to the frequent damage of the gut and the impaired absorption resulting from it, most patients need orthomolecular food supplementation until their intestinal mucosa is restored. This supplementation should also contain anti-oxidants.
A basic principle of naturopathic regulatory treatment of the tubercular constitution is that it can only be successful so long as the patient still has the ability to regulate. Furthermore it is absolutely necessary to support the excretion of body-waste and toxins released from the “Pischinger area” during the treatment.
According to Vithoulkas the three levels of the human being are closely interconnected and have to be treated simultaneously to be able to overcome the tubercular constitution. They are M (= mental-spiritual),
E (= emotional-psychological) and P (= physical and material).Besides treatment of levels M and E with adequate procedures (such as spiritual healing, breathing exercises, behaviour therapy, psychological support as a part of anthroposophical medical treatment), the basic treatment with medical preparations consists primarily in a combination of milieu therapy, (classical or complex-) homśopathy, biophoton activation, isopathy and immune modulation. Treatment with SANUM-medications (see “Isopathic/Homoeopathic Materia Medica”) forms an important connecting link between the material level P and the two non-material levels M and E.
By way of illustration, a medicinal milieu treatment for the regulative eradication of the tubercular constitution by Werthmann (Werthmann 1999) is described below. This basic therapy has proved its worth in the treatment of children and adults over many years. According to Werthmann, adults receive the following treatment:
1. Ubiquinone comp. (Heel) + CITROKEHL: Mixed injection i.m. once weekly
2. for two weeks: EXMYKEHL 3X Supp: evenings Monday - Friday; Saturday and Sunday
FORTAKEHL 5X one tablet to be taken twice3. after two weeks for some months: Monday - Friday: in the morning 1 tablet MUCOKEHL 5X, in
the evening 1 tablet NIGERSAN 5X, Saturday and Sunday twice daily 1 tablet FORTAKEHL 5X4. from the beginning of the second week: alternating daily SANUKEHL Myc 6X or SANUKEHL
Klebs 6X; 5 drops to be taken twice daily, plus 5 drops once daily for topical application5. starting in week 3: 1 capsule UTILIN “S” (weak or strong depending on the constitution) once
every 14 days6. acid-base regulation with ALKALA N and SANUVIS.
The mixed injection with Ubiquinone and other substances that contain “carbonyl-groups” as well as CITROKEHL serves to activate the photons in the cells and to enhance cell respiration. EXMYKEHL and FORTAKEHL help to re-establish the symbiosis of the gut and MUCOKEHL and NIGERSAN reverse the evolution of the high-valency forms according to Enderlein; SANUKEHL preparations stimulate the immune system to eliminate cell-wall-deficient forms of pathogenic micro-organisms (Cornelius, 1999; Schneider, 1999a; Werthmann, 1999). Finally, UTILIN “S” serves as a multi-potent immune-stimulant (Hartmann, 1990). Besides its general immune-stimulating property this preparation has a specific action in the eradication of the tubercular milieu. Therefore it is often used in the treatment of neoplastic diseases (Filion et al., 1999).
For the excretion of metabolic waste products and heavy metals from the “Pischinger area” the SANUM products CERIVIKEHL and especially USNEABASAN (Schneider, 1999b) are suitable; these are produced from lichens. The excretion needs to be enhanced for a few months; simultaneously the magnesium and zinc metabolism is regulated.
10 drops USNEABASAN (or CERIVIKEHL) should be taken in the morning, 1 capsule MAPURIT at lunchtime and 10 drops of ZINKOKEHL in the evening.
For the treatment of children the described basic treatment of the tubercular constitution is shortened and simplified (Werthmann, 1998b) as the ability to regulate is stronger then in adults. For infants of less then 1 year medication should not be administered orally if at all possible; instead topical application on the inner side of the elbow is recommended. Apart from this the dosage should be based on the number of years the child is old; one drop per year:
1. for 1 week once daily NOTAKEHL 5X drops or FORTAKEHL 5X drops for topical application or to be taken orally.
2. after that for several weeks: from Monday to Friday SANKOMBI 5X drops in the morning, Saturdays and Sundays NOTAKEHL 5X drops or FORTAKEHL 5X drops.
3. alternating daily 1-2 drops UTILIN N and RECARCIN N to be applied topically in the bend of the elbow.
4. in addition, classical homśopathic treatment with Thuja 6X.
The inherited or acquired tubercular constitution is a common cause of most chronic diseases. This had already been realised and written down by Hahnemann approximately 200 years ago. It has been confirmed by numerous other scientists such as Allen, Bernard, Béchamp, Enderlein and Reckeweg who investigated and clarified details. Although the existence of cell wall deficient variations (CWD) of pathogenic bacterial forms had initially not been recognised by conventional medicine, modern technology made it possible to show that they form an important substrate for this constitution. The triggering factor for the development of the tubercular constitution is mainly a change in the blood milieu and tissue milieu. Malnutrition plays an important part in the development of such a constitution. During the last 40 years generally suppressive measures in the form of chemical medication and vaccinations have become increasingly significant. After an improvement in diet and the removal of any obstacles to cure, the naturopathic regulatory therapy can in many cases successfully help to cure chronic illness by removing the tubercular constitution.
Allen, J.H.: Die chronischen Krankheiten – die Miasmen (Chronic diseases – the miasms); German translation by Renee von Schlick, 1996).
Arnoul, F.: Der Schlüssel des Lebens – Heilung durch biologische Therapie nach Professor Dr. Enderlein (The key of life - Healing through the natural therapy according to Professor Dr. Enderlein), Reichl, 1998.
Béchamp, A.: The blood and its third element; English translation from the French by M.A. Leverson, Kessinger Publishing Company, Montana, USA, 1912
Bergmann, V.A. and Boeckel, K.: Zur Diagnose der L-Formen der Bakterien aus Mastitiden (For the diagnosis of L-forms of bacteria from mastitis), Mh. Vet. Med. 44, 98-101, 1989
Beyer, D.: Resistente Bakterien – globale Herausforderung (Resistent bacteria – a global challenge); Gesundes Leben 6, 8-16, 1999
Bleker, M.-M.: Blutuntersuchung im Dunkelfeld nach Prof. Dr. Günther Enderlein (Blood analysis in the darkfield according to Prof. Dr. Günther Enderlein), 2nd edition, Semmelweis, 1997
Cornelius, P.: Nosoden und Begleittherapie (Nosodes and accompanying therapy), 3rd edition, Pflaum, 1999
Dechow, H.: Der Krebserreger ein Aspergillus (The aetiological agent for cancer – an aspergillus), Archiv der Entwicklungsgeschichte der Bakterien (Archive for the historical development of bacteria), 1 (2) 125-142, 1933
Elmau, H.: Bioelektronik nach Vincent und Säuren-Basen-Haushalt in Theorie und Praxis (Bio-electronics according to Vincent and the acid-alkaline economy in theory and practice); Haug, 1985
Enderlein, G.: Bakterien-Cyclogenie. Prolegomena zu Untersuchungen ueber Bau, geschlechtliche und ungeschlechtliche Fortpflanzung und Entwicklung der Bakterien (Cyclogeny of Bacteria. Prolegomena to a study of the structure, sexual and asexual reproduction and development of bacteria), Walter de Gruyter & Co, Berlin, 1925; reprint edition 1981 published by Semmelweis
Enderlein, G.: Über die potenzierte Vaccinebehandlung der Tuberkulose (On the treatment of tuberculosis with potentised vaccines), Immunobiologica 1 (2), 33-36, 1949
Enderlein, G.: Der Terminus Virus kein vergleichend-morphologischer Begriff (The term “virus” – not a comparative-morphological concept), Immunobiologica 1 (5/6), 188-192, 1954
Enderlein, G.: Akmon - Bausteine zur Vollgesundheit und Akmosophie, Bd. I-III, Ibica, 1955, 1957, 1959
Filion, M.C.P.; Lepicier, A. Morales and N.C. Philips: Mycobacterium cell wall complex directly induces apoptosis in human bladder cancer cells, Br. J. Cancer 79, 229-235, 1999
Fontes, A.: Bemerkungen über die tuberkulöse Infektion und ihr Virus. (Remarks on tubercular infection and its virus) Mem. Inst. Oswaldo Cruz 2, 141-146, 1910
Geison, G. L.: The private science of Louis Pasteur , Princeton University Press, 1997
Gerlach, F.: Krebs and obligater Pilzparasitismus (Cancer and obligate parasitic infestation with fungi), Urban & Schwarzenberg, 1948; reprint 1998 published by Semmelweis
Gries, F. A.: Der nicht insulinabhängige Diabetes mellitus (NIDDM, Typ II) (Non-insulin-dependant Diabetes mellitus) (NIDDM, type II), Bundesgesundheitsblatt 3/91, 125-128, 1991
Hahnemann, S.: Organon der Heilkunst (Organon of the Healing Art), 1st edition 1810, Hippokrates, 1982
Hahnemann, S.: Die chronischen Krankheiten, ihre eigentümliche Natur und homöopathische Heilung (The chronic diseases, their peculiar nature and their homeopathic cure), 1st edition 1828, Haug, 1994 (English edition: B. Jain, New Delhi, 1988)
Harmsen, H.: Zur Morphologie der Erreger der Tuberkulose (About the morphology of the causative agents of tuberculosis), Klinische Wochenzeitschrift 30, 817-819, 1952
Hartmann, J.: Mycobacterium phlei – multipotentes Immunstimulans , therapeutikon, 4, 474-483, 1990
Hoffmann, G. H., F. Nienhaus, H.-M. Poehling, F. Schönbeck, H. C. Weltzien and H. Wilbert: Lehrbuch der Phytomedizin (Textbook of Herbal Medicine), 3rd edition, Blackwell, 1994
Koch, W. F.: Das Überleben bei Krebs- und Viruskrankheiten – das Schlüsselprinzip ihrer Heilbarkeit (Surviving cancer and viral illnesses – the key principle to cure)
Kölmel, K. F., A. Pfahlberg, G. Mastrangelo, M. Niin, I. N. Botev, C. Seebacher, D. Schneider, D. Lambert, R. Shafir, E. M. Kokoschka, U. R. Kleeberg, B. M. Henz and O. Gefeller: Infections and melanoma risk: results of a multicentre EORTC case control study. Melanoma Research 9, 511-519, 1999
Kollath, W.: Die Ernährung als Naturwissenschaft (Nutrition as a natural science), Haug, 1967
Kobau, Chr.: Ganzheitlich und naturheilkundlich orientierte Zahnmedizin (Holistically and naturopathically orientated dentistry), Kobau, 1998 (available from the publisher Semmelweis-Verlag, Hoya)
Koerber, K. v., T. Männle u. C. Leitzmann: Vollwert-Ernährung. Grundlagen einer vernünftigen Ernaehrungsweise (Wholefood nutrition. Foundations of a sensible diet), 6th edition, Haug, 1987
Mattman, L. H.: Cell Wall Deficient Forms – Stealth Pathogens, 2nd edition, CRC Press, 1993
Mäkinen, K. K. and P. L. Mäkinen: Dependence of the dicarbonyl-sensitized photoinactivation of lactoperoxidase on irradiation wavelength, FEBS Lett 137: 276-278, 1982
Mielke, K. J.: Droge Wohlstandskost: chronisch krank durch Fehlernährung (Rich diet as a drug: chronically ill from malnutrition)
Pischinger, A: Das System der Grundregulation – Grundlagen für eine ganzheitsbiologische Theorie der Medizin (The system of basic regulation – foundations of a holistically biological theory of medicine), 8th extended edition, Haug, 1990
Popp, F. A., K. H. Li and Q. Gu: Recent advances in Biophoton Research and its applications, World Scientific, 1992
Rau, Th.: Isopathie: Milieukorrektur und SANUM-Therapie (Isopathy: Milieu adjustment and SANUM-Therapy)
Reckeweg, H.-H.: Homotoxikologie – Ganzheitsschau einer Synthese der Medizin (Homotoxicology – Holistic view of a synthesis of medicine), Aurelia, 1975
Reckeweg, H.-H.: Krebsprobleme (Cancer problems), 2nd enhanced edition, Aurelia, 1980
Schneider, P.: Multigenerationsstudie zur transplazentaren Wirksamkeit von 7, 12-Dimethylbenzanthracen bei C57BL/6-Mäusen (Multi generation study on the transplacental effect of 7, 12-Dimethylbenzanthracen in C57BL/6 mice), thesis, University of Hanover, 1981
Schneider, P.: Die Sanukehle – Polysaccharide zur Haptentherapie (The Sanukehls– polysaccharides for Hapten therapy), Semmelweis, 1999a
Schneider, P.: CERIVIKEHL und USNEABASAN – homöopathische Arzneimittel aus Flechten (CERIVIKEHL and USNEABASAN – homśopathic remedies produced from lichens), Sanum-Post 46, 7-8, 1999b
Schwerdtle, C. and F. Arnoul: Einführung in die Dunkelfelddiagnostik – die Untersuchung des Nativblutes nach Prof. Dr. Günther Enderlein (Introduction to dark-field diagnosis – the analysis of native blood using the method of Prof. Dr. Günther Enderlein) Semmelweis, 1993
Sears, P. M., M. Fettinger u. J. March-Salin: Isolation of L form variants after antibiotic treatment in Staphylococcus aureus bovine mastitis, J. Am. Vet. Med. Assoc, 191, 681-684, 1987
Selye, H.: Einführung in die Lehre vom Adaptionssyndrom (Introduction to the theory of the adaptation syndrome), Georg Thieme, 1953
Spengler, C.: Tuberkulose- und Syphilis-Arbeiten (Studies in Tuberculosis and Syphilis), H. Erfurt, Davos 1911
Vithoulkas, G.: Die neue Dimension der Medizin (A new Model of Health and Disease), 2nd edition, Wenderoth, 1998. (English edition: North Atlantic Books, Berkeley, Ca.)
Werthmann, K.: Ernährungsumstellung für chronisch Kranke und Allergiker. 2. Aufl. 1997. (Nutritional re-orientation for the chronically ill and allergy-sufferers.) (Obtainable from the publishers, Semmelweis-Verlag, Hoya.)
Werthmann, K.: Ratgeber für Allergiker und chronisch Kranke - Vorbeugung und Behandlung (Advice for allergic and chronic patients - prevention and treatment), ebi, 1998a (available from the publishers Semmelweis-Verlag, Hoya)
Werthmann, K.: Dermatosen – praxisnah betrachtet (dermatoses in practice), SANUM-Post 44, 2-5 1998b
Werthmann, K.: Die chancenreiche Therapie mit Sanukehlen – ein breites Wirkungsspektrum der Haptenpräparate (The promising treatment with Sanukehls - the broad-spectrum action of the hapten-preparations), SANUM-Post 48, 11-17, 1999
Windstosser, K.K.: Polymorphe Symbionten in Blut und Körpergewebe als potentielle Kofaktoren des Krebsgeschehens (Polymorphic symbionts in blood and body tissues as potential co-factors in carcinogenesis) Semmelweis, 1995
Worlitschek, M.: Praxis des Säure-Basen-Haushaltes. Grundlagen und Therapie. (Practice of the acid-base economy. Principles and Treatment), Haug, 1996