Iridology Course
This course has been given by Professor Bryan K Marcia
This is an interesting and interactive course that enables the student
to interact with one of the world’s most active researchers in
Iridology and Sclerology, Professor Bryan Marcia who earned his Ph.D.
in Iridology in the US. Students taking this course will be able to
really immerse themselves in thousands of images of human irides, along
with many real case histories. It will also be an honour and privilege
to interact with one of the world’s mentors in iridology who
will share their clinical experience with an open mind and a big, warm
heart.
The course is comprised of 15 levels, with comprehensive exams at the
end of each level that can be taken online. The 15 levels include:
Level One - Introduction to Iridology
This first level introduces the roots of Iridology going back to findings
in Tutankhamen's tomb toward current technological advancements and developments.
Results obtained by scientists especially during the last 15-20 years
have increased considerably our knowledge about the eyes complex exteroceptive
areas of reflected information, associated with the cerebral centers.
Level Two - Anatomy of the Eye - Iris Exam Procedures
This level covers basic anatomical fundamentals of the whole eye. Other
anatomical principles covered include the anterior part of the eye,
histology, bio-microscopic characteristics of the iris surface, physiological
functions of the iris, pathology of the anterior part of the eye, inborn
anomalies of the iris, diseases of the iris, benign tumors of the iris
and common pathology of the structures of the anterior eye will be
reviewed.
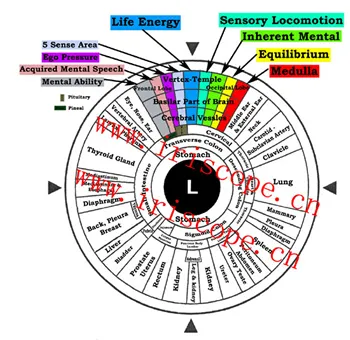
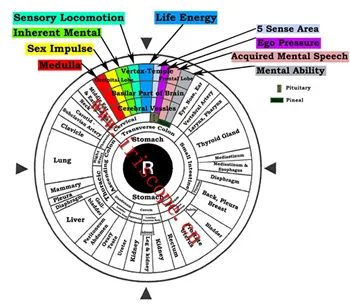
Level Three - Integrative Iridology Chart
One of the most controversial questions in iridology is the vast amount
(40 Plus) of Iridology charts. It has been distinguished that around
70% of iridology charts correspond with each other and around 25% have
unique differences. Students are shown how such topographical chart
differences can be justified by learning important factors. Several
Iridology charts from past centuries are shown to familiarize the student
with Iridology chart development. This level also covers detailed integrative
medicine recommendations for every topographic iris sector.
Level Four - Structural Signs of the Iris
Structural, reflex and pigment pathological signs are most informative
iridological signs. Students will discover how they provide the information
about the location of the pathological process, and allow, as far as
it is possible in iridology to evaluate their mechanism, stage, character
and severity.
Level Five - Constitutional Classification Via the Iris
This discipline will expose the student to numerous variations of iris
constitutions and associated treatment principles. From the standpoint
of prevention, the identification of a disease process in the pre-clinical
phase is more desirable than long-term therapy for damaged organs and
tissue systems. This can be achieved by accurately identifying the
constitution and the reactive capabilities of the patient with consideration
of environmental and stress factors.
Level Six - The Autonomic Nerve Wreath
The autonomic nerve wreath (ANW) is the projection of autonomous (vegetative)
nervous system. Students will discover how the Autonomic Nerve Wreath
has dual origin: embryological (from fetal membranes) and vascular
(from the vessels of the lesser arterial circle). The autonomic nerve
wreath is individual for each person; however, students will be shown
that it is possible to distinguish several typical forms including
its iridodiagnostic significance in detecting active genetic weaknesses.
Level Seven - Pupils and Pupillary Symptoms
The student will learn how pupil reflexes play the primary role in making
diagnosis of many neurological diseases, being a part of well-known
syndromes: Bernard-Horner, Adie's, Argylle-Robertson, Parinoud's etc.
Students will discover how changes of color, dimensions, shape, position
of center, equality and reflector reactions of pupils can have clinical
analysis significance.
Level Eight - Toxic Dystrophic Signs of the Iris
In this study, the student will learn about the group of toxic dystrophic
changes of iris and how Iridodiagnostic tests make it possible to evaluate
many toxic-dystrophic processes. Students will also discover how toxic-dystrophic
signs are symptoms of organism changes and how to offer pertinent lifestyle
recommendations.
Level Nine - Heterochromias of the Iris
Students will learn about heterochromias of iris and differentiation
between inherited and acquired diffuse and local changes of color.
Students will discover the importance of hereditary peculiarities of
iris color, toxic and drug dyschromias, pigment spots and their color,
tints of iris stroma and why they should be carefully analyzed.
Level Ten - Adaptive Rings and Arcs
Ophthalmologists consider contraction rings to be the simple folds of
the iris, and explain their origination by the work of neuro-motor
apparatus of the eye and its contraction, dilation of the superficial
layers in the iris. However, iridologists believe that some other factors
should be taken into consideration since not everyone has such rings
and arcs! This level will explore several theories why such rings and
arcs occur in the iris.
Level Eleven - Pigment spots in the Iris
It is considered that pigment spots always point to the pathological
process in the organism thereby they belong to the very important topic
diagnostic signs of iris. Students will learn how residual spots are
indicative of the end of pathological process in the associated organ
and how their colors, size, form, density are important indicators
for clinical evaluation.
Level Twelve - Conjunctiva Signs
The Student will learn how evaluation of bulbar conjunctiva does not
duplicate the iridodiagnostic examination but can offer entirely new
data to the results of iridodiagnostics.
Level Thirteen - Iridological Axis Signs
Axis signs consist of a group of markers consisting of lacuna, crypts,
radial furrows, pigment and collarette signs found in specific locations
in the eye. The student shall learn how to recognize possible irido-reflex
markers in the eye.
Level Fourteen – Transversals in the Iris
Transversals are very important focus signs in the iris for the student
to learn. Transversals can point to possible tissue change and congestion
in the corresponding organ. Students will review actual clinical examples
of the several possible types of transversals that can appear in the
iris.
Level 15 - Iridodiagnostic Examination Procedures
Students will learn how iridodiagnostic conclusion is made according
to the appearance of the iris and its signs, thereby basing iridodiagnostic
methods on visual and iridoscopic examination of the iris. Devices
used for iridological examination procedures including expert evaluation
of iris signs are covered in great detail.
*All courses include three iridological charts, student web server database
access (on-line videos, case studies, searchable databases), lifetime
account access.
Course Requirements
There will be some additional reading material and time spent researching
the many resources on the website. Studying some of the case histories
is also important. The serious professional would also be interested
in investing a little more and buying a professional iridoscope that
will enable you to capture your patient’s irides on the computer
screen and analyze and diagnose using sophisticated software which
also produces professional reports for your patients to take away with
them.
Course Goals and Objectives
This course will present a comprehensive overview of the Iridological
sciences while exploring the continuum of research & development
ranging from existing Iridodiagnostic principles to current theories
and applications. Students will additionally explore the implications
of utilizing Iridology as an adjunctive diagnostic modality in North
America. This course will examine contemporary issues such as the relationship
between North American Iris Analysis and several European-Asian Iridodiagnostic
principles.
The student shall be able to demonstrate knowledge about Iridology in
both historical and contemporary context.
To have the student understand the Central Hypotheses of Iridology.
Expose students to specific techniques of iris reading and begin to
practice using a magnifying lens, camera systems and digital iriscope
systems.
To instruct students with difficult iris analysis techniques such as
brown and highly pigmented eyes.
To teach how pupil reflexes play a primary role in many neurological
diseases.
Assist the student in understanding the similarity and differences between
American/Jensen Iridology research and current research accomplished
in Europe and Asia.
Students will study modern concepts of physiology and doctrine regarding
nerve activity and theories.
Students will discover the significance of the eccentric adaptive rings
in the iris.
Students will discover the iridodiagnostic significance in detecting
a genetically active weakness via the Autonomic Nerve Wreath.
The student will learn about the classifications of toxic dystrophic
changes of iris.
Students will discover how structural, reflex and pigment pathological
signs are the most informative Iridological signs regarding the location
of certain pathological processes in the body.
Students will identify changes of pupil color, dimensions, shape, position,
equality and reflector reactions and their clinical significance.
Students will learn how residual spots found in the iris are indicative
of the end of pathological process of an associated organ.
Students will learn how visible changes of conjunctiva vessels, crystalline,
cornea can add to Iridological conclusions.
Students will discover the importance of hereditary peculiarities in
iris color including toxic and drug dyschromias, pigment spots and their
color.
To expose the student to numerous variations of iris constitutions and
associated treatment principles.
To offer student clinical and educational forms for use in clinical
practice.
To maintain student motivation and activity throughout their course
learning process.
To expose the student to the most current Iridological research developments.
To guide students through complete iris analysis.
To have the student successfully pass examinations.
Course Materials
All the course material required to complete this course is contained
in this course. This will include CDs and DVDs that will load the complete
course onto your computer so that you can access it anywhere in the
world. Once installed, there are many interactive links that enable
you to research to your hearts content many aspects of iridology and
sclerology. The serious practitioner will also want to order the iridoscope
with computer software to begin examining their patient’s irides
immediately.
Grading Policy
Each lesson is followed by an end of lesson exam which will be based
on material covered in the lesson.
Recommended Books
All course material is given online. There are no required books for
this course but here are a few recommended titles for additional study.
What is Iridology?
Iridology is the study of the iris of the eye.
There are many theories on how Iridology indicates what is going on
in the body. To understand the theories you may also want to research
reflexology, acupressure and acupuncture.
One is a theory that there are hundreds of thousands of nerves or energies
running from every tissue and organ of the body, ending in the tips of
your fingers and toes as well as the iris of your eyes. That is why stubbing
your toes hurts more than the same impact on the leg.
Nature is somewhat constant. Most people know that when the roots of
a plant have been injured or aren't receiving the nutrients or moisture
that they need, the first signs of the decline in the health of the plant
will be found in the outer most part of the leaves.
Apply that to the nerve endings that are running throughout your body.
If, for instance, your pancreas has been damaged or lacking a nutrient
or is in poor health, the first sign of the decline in the health of
the pancreas will be found in the outermost part of the nerve endings,
many which end in the iris of the eye.
Though exact neurological mechanics of the phenomenon is not fully understood,
it seems that when an organ or body system is in poor health the nerve
running from that body part will start to recede, somewhat like a leaf
wilts. When it does, it draws with it various degrees of the layers of
fibers which make up the color of the iris of the eyes, leaving darkened
marks called lesions.
Traditional medicine
What is traditional medicine?
Traditional medicine refers to health practices, approaches, knowledge
and beliefs incorporating plant, animal and mineral based medicines,
spiritual therapies, manual techniques and exercises, applied singularly
or in combination to treat, diagnose and prevent illnesses or maintain
well-being.
Countries in Africa, Asia and Latin America use traditional medicine
(TM) to help meet some of their primary health care needs. In Africa,
up to 80% of the population uses traditional medicine for primary health
care. In industralized countries, adaptations of traditional medicine
are termed “Complementary“ or “Alternative” (CAM).
Increasing use and popularity
TM has maintained its popularity in all regions of the developing world
and its use is rapidly spreading in industrialized countries.
In China, traditional herbal preparations account for 30%-50% of the
total medicinal consumption.
In Ghana, Mali, Nigeria and Zambia, the first line of treatment for 60%
of children with high fever resulting from malaria is the use of herbal
medicines at home.
WHO estimates that in several African countries traditional birth attendants
assist in the majority of births.
In Europe, North America and other industrialized regions, over 50% of
the population have used complementary or alternative medicine at least
once.
In San Francisco, London and South Africa, 75% of people living with
HIV/AIDS use TM/CAM.
70% of the population in Canada have used complementary medicine at least
once.
In Germany, 90% of the population have used a natural remedy at some
point in their life. Between 1995 and 2000, the number of doctors who
had undergone special training in natural remedy medicine had almost
doubled to 10 800.
In the United States, 158 million of the adult population use complementary
medicines and according to the USA Commission for Alternative and Complementary
medicines, US $17 billion was spent on traditional remedies in 2000.
In the United Kingdom, annual expenditure on alternative medicine is
US$ 230 million.
The global market for herbal medicines currently stands at over US $
60 billion annually and is growing steadily.
Safety and efficacy issues
Scientific evidence from randomized clinical trials is only strong for
many uses of acupuncture, some herbal medicines and for some of the manual
therapies. Further research is needed to ascertain the efficacy and safety
of several other practices and medicinal plants.
Unregulated or inappropriate use of traditional medicines and practices
can have negative or dangerous effects.
For instance, the herb “Ma Huang” ( ) is traditionally used
in China to treat respiratory congestion. In the United States, the herb
was marketed as a dietary aid, whose over dosage led to at least a dozen
deaths, heart attacks and strokes.
In Belgium, at least 70 people required renal transplant or dialysis
for interstitial fibrosis of the kidney after taking a herbal preparation
made from the wrong species of plant as slimming treatment.
Biodiversity and sustainability
In addition to patient safety issues, there is the risk that a growing
herbal market and its great commercial benefit might pose a threat to
biodiversity through the over harvesting of the raw material for herbal
medicines and other natural health care products. These practices, if
not controlled, may lead to the extinction of endangered species and
the destruction of natural habitats and resources.
Another related issue is that at present, the requirements for protection
provided under international standards for patent law and by most national
conventional patent laws are inadequate to protect traditional knowledge
and biodiversity.
Tried and tested methods and products
25% of modern medicines are made from plants first used traditionally.
Acupuncture has been proven effective in relieving postoperative pain,
nausea during pregnancy, nausea and vomiting resulting from chemotherapy,
and dental pain with extremely low side effects. It can also alleviate
anxiety, panic disorders and insomnia.
Yoga can reduce asthma attacks while Tai Ji techniques can help the elderly
reduce their fear of falls.
TM can also have impact on infectious diseases. For example, the Chinese
herbal remedy Artemisia annua, used in China for almost 2000 years has
been found to be effective against resistant malaria and could create
a breakthrough in preventing almost one million deaths annually, most
of them children, from severe malaria.
In South Africa, the Medical Research Council is conducting studies on
the efficacy of the plant Sutherlandia Microphylla in treating AIDS patients.
Traditionally used as a tonic, this plant may increase energy, appetite
and body mass in people living with HIV.
WHO efforts in promoting safe, effective and affordable traditional medicine
The World Health Organization launched its first ever comprehensive
traditional medicine strategy in 2002. The strategy is designed to assist
countries to:
Develop national policies on the evaluation and regulation of TM/CAM
practices;
Create a stronger evidence base on the safety, efficacy and quality of
the TAM/CAM products and practices;
Ensure availability and affordability of TM/CAM including essential herbal
medicines;
Promote therapeutically sound use of TM/CAM by providers and consumers;
Document traditional medicines and remedies.
At present, WHO is supporting clinical studies on antimalarials in three
African countries; the studies are revealing good potential for herbal
antimalarials.
Other collaboration is taking place with Burkina Faso, the Democratic
Republic of the Congo, Ghana, Mali, Nigeria, Kenya, Uganda, and Zimbabwe
in the research and evaluation of herbal treatments for HIV/ AIDS, malaria,
sickle cell anaemia and Diabetes Mellitus.
In Tanzania, WHO, in collaboration with China, is providing technical
support to the government for the production of antimalarials derived
from the Chinese herb Artemisia annua. Local production of the medicine
will bring the price of one dose down from US $6 or $7 to a more affordable
$2.
In 2003, WHO support has so far facilitated the development and introduction
of traditional and alternative health care curricula in seven tertiary
education institutions in the Philippines.
Training workshops on the use of traditional medicines for selected
diseases and disorders have also been organized in China, Mongolia and
Vietnam.
Priorities for promoting the use of traditional medicines
Over one-third of the population in developing countries lack access
to essential medicines. The provision of safe and effective TM/CAM therapies
could become a critical tool to increase access to health care.
While China, the Democratic People’s Republic of Korea, the Republic
of Korea and Vietnam have fully integrated traditional medicine into
their health care systems, many countries are yet to collect and integrate
standardized evidence on this type of health care.
70 countries have a national regulation on herbal medicines but the
legislative control of medicinal plants has not evolved around a structured
model. This is because medicinal products or herbs are defined differently
in different countries and diverse approaches have been adopted with
regard to licensing, dispensing, manufacturing and trading.
The limited scientific evidence about TM/CAM’s safety and efficacy
as well as other considerations make it important for governments to:
Formulate national policy and regulation for the proper use of TM/CAM
and its integration into national health care systems in line with the
provisions of the WHO strategies on Traditional Medicines;
Establish regulatory mechanisms to control the safety and quality of
products and of TM/CAM practice;
Create awareness about safe and effective TM/CAM therapies among the
public and consumers;
Cultivate and conserve medicinal plants to ensure their sustainable use.
Recommendations by WHO and EU
The WHO Traditional Medicines Strategy 2002-2005 outlines the role and
activities in traditional medicines / complementary and alternative medicine
(TM/CAM) (ref 1). The strategy incorporates four objectives, two of which
focus on safety:
Policy – Integrate TM/CAM with national health care systems, as
appropriate, by developing and implementing national TM/CAM policies
and programmes.
Safety, efficacy and quality – Promote the safety, efficacy and
quality of TM/CAM by expanding the knowledge-base on TM/CAM, and by providing
guidance on regulatory and quality assurance standards.
The European Union (EU) treaty came into force on November 1 1993. The
treaty was intended to open a large market zone without borders, enabling
the free movement of persons, goods, services, and capital. The treaty’s
regulation of movement of persons and goods affects in particular health
service and medications. WHO gives the following description in the "Legal
status of TM/CAM: A worldwide review":
Although the free movement of persons within the European Union is the
cornerstone of the Treaty of Rome, the diversity of national policies
severely limits its applicability to practitioners of CAM. Case 61/89
of the European Court of Justice involved an acupuncturist without allopathic
medical qualifications practising in France. The courts decision confirmed
the right of individual countries to make their own legislation on whether
or not to reserve the practice of medicine to allopathic doctors.
Nonetheless, in April 1994, European Deputy Paul Lannoye presented a
proposal on the status of CAM to the European Parliament Committee on
the Environment, Public Health, and Consumers Protection. He asked for
provisions for CAM within social security systems, the incorporation
of CAM into the European Pharmacopoeia, an end to prosecutions of non-allopathic
practitioners in the countries where the practise of medicine is the
exclusive domain of allopathic providers, and a pan-European system of
recognition and regulation of CAM practitioners along the lines of the
British Osteopath and Chiropractor Acts. He also requested a research
budget of 10 million Euros per year for five years. At the last moment
the European Parliament cancelled the vote on the proposal (ref 2).
In May 1997 The European Parliament adopted a resolution on the status
of non-conventional medicine (ref 3). The resolution called the Commission
to:
Launch a process of recognising non-conventional medicine.
Carry out a thorough study into safety, effectiveness, area of application
and the complementary or alternative nature of all non-conventional medicines
with a view to their eventual legal recognition….
Draw up a comparative study of the various national legal models to which
non-conventional medical practitioners are subject….
In formulating European legislation … make clear distinction between
non-conventional medicines that are "complementary" in nature
and those which are "alternative" medicines in the sense that
they replace conventional medicine…
A resolution of the European Parliament, however, is not a binding act,
but a declaration of policy. Nonetheless, the adoption of the resolution
has led several countries to consider revising legislation (ref 4).
Concerning CAM providers and CAM therapies, an EU resolution in 1999
stated:
"
In the health field, it is important to preserve the diversity of national
legislation and practise that is one of Europe’s assets: people’s
attachment to their own systems and tradition must not be called into
question. Nevertheless, the Assembly believes that a common European
approach to non-conventional medicine based on the principle of patients’ freedom
of choice in health care should not be ruled out."
"
The Assembly believes that the best guarantee for patients lies in a
properly trained profession, which is aware of its limitations, has a
system of ethics and self-regulation and is also subject to outside control." (ref
5)
This resolution and case 61/89 of the European Court of Justice gave
the members of the European Union the opportunity to regulate CAM therapies
and providers according to health legislation and CAM tradition in their
own countries.
The EU parliament has, since 1994, adopted several directives regulating
the trade of herbal products. Two directives concerning homeopathy came
into force on January 1994: one applicable for homeopathic products for
humans and one applicable for homeopathic veterinary products. The directive
on traditional herbal medical products will be in force from 1 November
2005 (2004/24/EC), and the directive on food supplements was set in force
from 1 August 2005 (Vitamins & Minerals, 2002/46/EC). These directives
will be adopted in the legislation of the European countries and will
thus harmonize the regulation of herbal products and food supplements.
References
1. WHO, Traditional Medicine Strategy 2002-2005 (document WHO/EDM/TRM/2002.1).
Geneva: World Health Organization, 2002.
2. Legal Status of Traditional Medicine and Complementary/Alternative
Medicine: A Worldwide Review, (document WHO/EDM/TRM/2001.2). Geneva:
World Health Organization, 2001: s 188.
3. European Parliament, Resolution A4 1997/0075.
4. Legal Status of Traditional Medicine and Complementary/Alternative
Medicine: A Worldwide Review, (document WHO/EDM/TRM/2001.2). Geneva:
World Health Organization, 2001.
5. European Parliament Resolution 1999/1206
|