Live-blood Analysis
If you take a small drop of blood from a finger tip and place it on a slide under a darkfield microscope you can watch patterns in the live-blood. In standard microscopy light is shone directly through the sample (specimen) and viewed against a bright field or background. However, we cannot easily observe live material in this manner. Because a specimen must be thin to be observed, it is also virtually transparent. Therefore we must stain it to see it, and to do this we usually have to kill the specimen. This staining process has become very sophisticated. There are hundreds of stains and hundreds of questions you can ask about your specimen with these stains. And that, as far as most microscopists are concerned, is that. 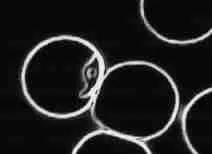
With darkfield microscopy, however, the procedure is crucially different. The light does not travel directly through the specimen, but comes in from the sides and only light which is reflected by the specimen is viewed and viewed against a dark background, hence ?arkfield microscopy? In this way a highly contrasted image is obtained and there is no need to use a stain. We can therefore watch living material. 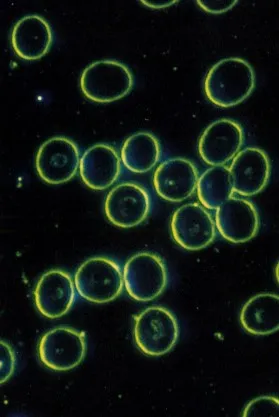
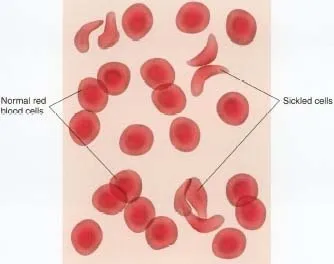
Quebec scientist Gaston Naessens is a controversial figure who invented a remarkable microscope using a complex UV light source. He called it a "somatoscope" and with it he was able to examine living material at 30 times the resolution available with conventional microscopes. This led him to the discovery of what he calls "somatids". Somatid means "tiny bodies". According to Naessens somatids are found in all living creatures. In a healthy organism somatids have a simple three stage life cycle (somatid, spore, and double spore). In this "microcycle" somatids are symbiotic: they perform essential functions in the regulation of cell division, Naessens claims. However, when we are ill the somatids elaborate into a complex sixteen stage "macrocycle". The somatids of the macrocycle are bacteria-like and fungus-like. This change of form is an example of what is called "pleomorphism". Gaston Naessens' theory says that we see the macrocycle in ill health or with impending illness. It is also claimed that with the darkield microscope we may see the disease pattern in the blood up to two years before a disease (for example cancer) manifests. The somatid cycle (discovered by Naessens with the somatoscope and analyzed in culture) can be observed and monitored with darkfield microscopy. We can use this to alert us to incipient problems, or to monitor a patients response to therapies, both orthodox or alternative therapies. A second approach to live-blood analysis has been assembled from many sources by Prof. Lida Mattman of the Wayne State University and her colleague Dr. Phil Hockstra. Micro-organisms, when challenged, shed their cell walls. While this leaves them less virulent, it also makes them less vulnerable. Shedding their skins they lose most of the markers that identify them as foreign bodies to our immune systems. They can also now change their shape - this simple change of shape is also called pleomorphism - and all this means they can easily invade and hide in the body's own cells. In live-blood analysis as taught by Dr. Hockstra attention is paid to the microbes, to the shape and activity of the white blood cells (WBC) and red blood cells (RBC). By observing the red cells we can tell a lot about the state of metabolism in general and of the liver particular. Meanwhile, observing the white cells gives us a reading on the state of the immune system, and the pattern of microbes tell us if disease is overwhelming the body's defences. Note that while we call this "live-blood" analysis it is really dying blood that we are observing. In a sense we are watching how quickly rot sets in after we take the drop of blood out of the body and this tells us how much resilience and vitality there is in the body - it is a measure of the body's health. 
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Live Blood Analysis Diploma Course WHAT
ARE WE SEENG UNDER THE DARKFIELD MICROSCOPE: INTERPRETING THE BLOOD MORPHOLOGIES
CLASSICAL MICROBIOLOGICAL VIEWLESSON 8 – PART I INTRODUCTION There
are two ways to answer the question in the title of this lesson: What
are we seeing under the darkfield microscope? How do we interpret these
morphologies that we see? Prof. Enderlein spent many years observing
morphologies under the microscope and indeed in those days the technology
was much less developed that it is today. Most darkfield microscopists
usually study the Enderleinian perspective and analyze the blood according
to this. Whether this is right or wrong is a difficult judgement. What
I am convinced about, however, having read much of the Enderlein research
and compared it to more modern research to try to understand what is
being seen under darkfield, I have come to the conclusion that both sides
present interesting data. However, if I were in a court of law with a
traditionally trained microbiologist trying to defend Enderleinian principles,
I would be on very shaky ground indeed! Modern microbiologists do not
recognize the morphologies or the language used by Enderlein and as expert
witnesses in a court of law, their word counts. However, there is the
more traditional, scientific approach that microbiologists would understand
and agree with the various morphologies seen in darkfield – here
you will be on safe, scientific ground as you are simply using your darkfield
microscope as a scientist identifying various morphologies and interpreting
according to traditional microbiological knowledge. In this course I
do not intend to omit either of these two views – if anything,
the Enderlein perspective has important historical significance, but
on the other hand science is not set in stone and I strongly believe
that more work in this field of live blood analysis will reveal a lot
that is not part of our knowledge base at the moment. Therefore, Enderlein’s
perspective will be given, along with a number of his own papers for
those that want to pursue his research further and get a better understanding.
Most of these papers are in Lessons 4 and 5 which talks about the history
of darkfield microscopy as well as the work of Prof. Enderlein. This
lesson I have left more for those that want to feel safe in that court
of law so thatthey can be on the same page as the traditional microbiologist.
Everything that you interpret in the blood picture that you see under
darkfield, based on what you learn from this lesson, is scientific and
well-researched and understood by most microbiologists. So let’s
begin our learning in this fascinating field of darkfield microscopy
and get some real science under our belt! TRADITIONAL MICROBIOLOGY & HAEMATOLOGY
In traditional haematology and microbiology, there is much research on
the various components of blood. These blood components have been correlated
with other biochemical tests, as well as various disease processes. © Dr.
George J Georgiou, Larnaca, Cyprus, 2008
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
IMPORTANCE OF DARK-FIELD EXAMINATION IN EARLY DIAGNOSIS AND TREATMENT OF SYPHILIS by M. P. Vora, M.B.B.S. HON. CLINICAL ASSISTANT, VENEREAL DEPT., SIR J. J. HOSPITAL, BOMBAY. The Medical Bulletin Number. 2 of Volume No –VIII.,1940, Number. 182 of January 20 th, 1940. Page No. 40 to 42. Dark-field examination is a valuable means of diagnosing syphilis in its very early stage. It is a method by which one can directly observe and identify the Treponema pallidum in the living condition. Once one is familiarized with the characteristics of the Treponema pallidum it is not likely to be mistaken for anything else. Its recognition is always conclusive. Dark-field examination is very simple and can be done in a short time on a good bacteriological microscope with a special dark-field condenser. The technique is easy and can be mastered in a short time. The detection of the Treponema pallidum in the serous exudate from the chancre is pathognomonic of Lues, though failure to find at one examination does not exclude the infection. The organism, though always present, in the primary lesion may not be found at once and careful and repeated searches may be necessary. The results of the examination are accurate and compare well with other diagnostic procedures. Dark-field examination is also of considerable value in diagnosing Wassermann-negative secondary syphilis. In this examination there are not the same difficulties of interpretation, or fallacies as one has in the Wassermann reaction, which also takes some time to develop. Hence this method of diagnosis can be applied with advantage in cases of early syphilis. Great importance of early diagnosis and early institution of specific treatment in syphilis cannot be disputed; for earlier the treatment is started the greater the hope of complete cure. Besides, early diagnosis will curtail the prolonged illness and reduce the length of the courses of treatment. It also means saving some inconvenience and expenses both to the patient and the hospital. It will help to control the transmission and the spread of infection which is inevitable otherwise. Upon this will depend our best hope of eradicating the disease, an important problem in Public Health. The tendency to wait till the Wassermann reaction proves positive is to be deplored. Usually one has to wait for a few (4 to 8) weeks before the test becomes positive- a period in which the diagnosis can be easily established in the majority of the cases by the dark-field examination. The percentage of positive Wassermann reactions increases with the age of the disease until the secondary stage is established whereas the percentage of the dark-field examinations reaches in the maximum in the second week of the appearance of the sore. In expert hands, during the second week, the results of the former have been calculated to be about 35%, while those of the latter procedure attain a figure of over 90%. “In subjecting a patient with venereal sore to a Wassermann reaction one must clearly understand that so far as the diagnosis is concerned one is employing a method which is at it’s worst precisely at a time when the dark-field examination is at its best. It means deliberate sacrifice of the patient’s chance of complete cure.” Taking these facts into consideration and also bearing in mind the frequency of the positive results with a dark-field examination, the value of this test increases proportionately and ranks high in importance. It is very unfortunate that such a simple and reliable method of diagnosing syphilis should have sustained delay in popularization. The Material – The follow-up of the cases studied is not very satisfactory, because several of the patients who attend the clinic sadly lack any sense of co-operation. Few patients give a proper history or follow regular treatment to completion. A series of 120 patients, clinically diagnosed as suffering from venereal sores were subjected to dark-field examination and Wassermann reaction in the first week of their attendance in the V.D. Department of the Sir J. J. Hospital. The exact day of the appearance of the sore could not be found out in the majority of cases. The cases which were Wassermann negative in the first instance were again subjected to a Wassermann test a second time in the third week. Further follow-up was not possible because some had their treatment started, while others failed to attend. Reports of five of the cases were not available for reference. The 115 cases fall into the following groups:- TABLE –I
TABLE –II
TABLE –III Wassermann results with reference to the results of the Dark-field examination
TABLE –IV
The study of the above tables will show the following important points:
As regards the treatment, the maximum amount of treatment necessarily required in a given case will undoubtedly vary; but even in those cases who start and follow regular treatment in the sero-negative primary stage, the minimum is necessary both in amount and time. Two or three courses of specific treatment will be adequate for cure in the majority of cases instead of four minimum after all signs and symptoms have disappeared when the Wassermann reaction becomes early positive, i.e. two years’course. A course means ten injections each of N.A.B. and Bismostab in moderate doses given regularly at weekly intervals. By this it is not meant to suggest any short or abortive form of treatment. Twenty injections each of arsenic and bismuth, probably more but not less, are fundamental to the control of syphilis in its very early stages. It could not be overemphasized that under no circumstances should the so-called abortive cure by short treatment followed by series of blood tests be considered adequate and worthy of trial; for syphilis is a relapsing disease par excellence and every consideration of its cure and prognosis must be based on this qualification.”It is this feature that renders Lues so serious. Syphilologists should spare no efforts to impress on the minds of the patients the fact that the treatment must be pursued even though the lesion have healed and the Wassermann reactions have become negative. No case should be dismissed as cured unless and until repeated examinations of blood, cerebro-spinal fluid, skin and mucosa show persistent negative results. Cerebro-spinal fluid is examined not only for Wassermann reaction but also for increase of proteins, especially globulins and the cell-count. This is the only way to check the significant and extensive problem that confronts modern medicine. An argument is sometimes advanced against this early treatment. It is said that it prevents ‘healthy reaction’which is natural in the development of the disease, that it impairs the resistance of the individual and that it makes relapse or recrudescence commoner. This argument is not convincing; for there are a few cases in which a relapse is inevitable notwithstanding the fact that the cases started late treatment and followed it religiously to completion. If immunity is to develop it should do so by the time the sore appears, i.e. during the incubation period for three or more weeks, long before which the organisms completely invade the human body. Relapse- it looks reasonable- should be attributed to improper treatment, to the failure to use heavy metal with arsenic, to the tendency to attach too much importance to blood tests alone and lastly to the relapsing nature of the disease. Careful analysis of the cases will be convincing. Practically no case should relapse i.e. show signs of syphilis and become sero-positive if every case is diagnosed early, is given regularly the proper treatment and is followed up by constant observation. Relapse should become a myth and complete cure can be assured generally. Conclusions – “The results of treatment commenced in the sero-negative primary stage are overwhelmingly superior to those begun later. It is therefore of the utmost importance to establish the diagnosis of syphilis before the advent of positive Wassermann reaction and this can only be done with certainty by finding Treponema pallidum in the serum expressed from the primary sore.”Hence dark-ground examination should be made as a routine in every case of venereal sore and the golden opportunity of treating the disease in its early and curable stage should not be lost. It would indeed be an invaluable contribution towards the treatment and relief of the syphilitics. Acknowledgement – I am especially indebted to Dr. W. N. Weliker, Venereologist, Sir J. J. Group of Hospitals, for kindly permitting me to follow and publish the reports of the cases and Professors P.V. Gharpure and M. J. Parmanand for helping me and giving me the facilities to carry out this work and to Lt-Col. Jelal M. Shah I.M.S. for his encouragement.
REFERENCES STOKES, Modern Syphilology. CONYBEARE, Text Book of Medicine. HARRISON , Venereal Diseases. DAVID LEES, Diagnosis and Treatment of Venereal Diseases. |
 This
is a normal function of blood and, furthermore, its extent cannot be
easily quantified with live-blood work. (This is because we can not calculate
exactly how thick the sample is at any point.) The extent of this clumping,
this rouleaux formation can however be easily measured in standard blood
work as sedimentation rate, or SED rate. (If rouleaux formation is excessive
the blood sediments settle more quickly.) SED rate is a general indicator
of inflammation. We generally expect the SED rate to be elevated in inflammatory
conditions such as arthritis. But SED rate is a very general and imprecise
measure, and medicine pays little attention to it nowdays.
This
is a normal function of blood and, furthermore, its extent cannot be
easily quantified with live-blood work. (This is because we can not calculate
exactly how thick the sample is at any point.) The extent of this clumping,
this rouleaux formation can however be easily measured in standard blood
work as sedimentation rate, or SED rate. (If rouleaux formation is excessive
the blood sediments settle more quickly.) SED rate is a general indicator
of inflammation. We generally expect the SED rate to be elevated in inflammatory
conditions such as arthritis. But SED rate is a very general and imprecise
measure, and medicine pays little attention to it nowdays.